



By Diana Koklonis, Health Professionals Liaison Team Manager at Optibac Probiotics, BNutDiet (Hons), MSc and Dr Kate Steed, Scientific Training Manager at Optibac Probiotics, Medical Microbiologist PhD
In this blog, we explore the overlap between Irritable Bowel Syndrome (IBS) and Inflammatory Bowel Disease (IBD) in clinical practice and examine how the gut microbiome and probiotics may support management of these conditions. Within the blog, you’ll find insights and practical guidance to help navigate the challenges of these digestive disorders.
What is IBS and IBD? What is the criteria for diagnosis? Let’s recap first –
IBS is a functional bowel disorder characterised by recurrent abdominal pain linked to defecation or changes in stool frequency and form. There are no structural changes nor visible inflammation. Diagnosis is based on symptoms and excluding other conditions 59,12.
In contrast, IBD is a chronic inflammatory disease with visible gastrointestinal mucosal inflammation and lesions. It involves abnormal immune activation in genetically susceptible individuals and is normally diagnosed through stool testing and colonoscopy with biopsies. The two main types of IBD are ulcerative colitis (UC) and Crohn’s disease (CD). Symptoms include abdominal pain, diarrhoea, rectal bleeding, fatigue and weight loss43,17.
While distinct, an overlap between the two has been noted, with the gut microbiome and inflammation suggested as risk factors.
What is an overlap between IBS and IBD? An overview.
The overlap refers to the prevalence of IBS-like symptoms in IBD patients who are in remission, with some researchers suggesting the co-existence of both conditions. However, others argue that mucosal inflammation in IBD may mimic IBS symptoms, as the gastrointestinal tract has a limited range of symptom manifestations, leading to similar presentations like abdominal pain, bloating, and diarrhoea12.
Why is understanding the IBS-IBD overlap important?
Understanding the overlap is crucial for clinical practice as it could impact the diagnosis and treatment strategies. Research shows that up to 40% of IBD patients experience persistent gastrointestinal symptoms, even during histological remission, which fit IBS criteria and cannot be explained by IBD alone.
Could IBS and IBD coexist? or lead to one another? Let’s have a look at some stats from the clinical evidence:
- An observational study with 9,341 IBS and 18,678 non-IBS cases found an 8.6-fold incidence (p < 0.0001) of IBD among those with IBS52although the number of people with a first degree relative with IBD was not reported in this study.
- A cross-sectional study found that 27.7% patients with CD and 19.8% with UC had true IBS-type symptoms in the absence of mucosal inflammation16.
- An observational study found a 35% incidence of IBS-like symptoms in UC patients with active inflammation and 29% in those in remission.21
- A meta-analysis found that 32.5% of IBD patients had IBS symptoms. Prevalence was lower during remission (23.5%)27.
- A Mendelian randomization study (2023) found that people with a genetic risk for IBD had a greater genetic risk for developing IBS (OR 1.2), however genetic risk for IBS did not indicate greater risk of developing IBD.
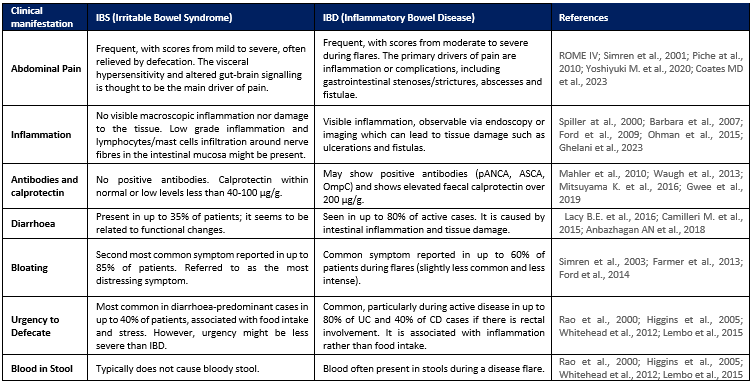
IBS vs. IBD: Similarities and Differences
IBS and IBD share several similarities, including symptoms, demographics and risk factors. But there are also several differences. Let’s explore some of them:
Is there a role of the gut microbiome in the pathogenesis of IBS, IBD and its overlap?
IBD: Pathogenesis is driven by the interaction of gut microbiota, the immune system, genetics, and environmental factors. The disease phenotype cannot be explained by genetics alone, and the gut microbiome is thought to play a key role. IBD-associated genes may trigger an exaggerated immune response against gut microbes, leading to persistent immune activation. There is a strong degree of dysbiosis in IBD, more so than IBS. This may explain why the microbiome in IBD has been linked to disease severity and poorer treatment outcome, as well as its use as a diagnostic tool.28,43,1,17,55,15,51,76,19
The gut microbiota in IBD shows a reduced diversity (not unanimously accepted) with a significant decrease of beneficial bacteria such as Bifidobacterium spp. ,Lactobacillus spp., and Faecalibacterium prausnitzii 48,24,2, and a higher abundance of pathogens such as Escherichia coli and Clostridioides difficile.58 Increased numbers of antibodies against the E. coli outer membrane were detected in 37 to 55% of patients with CD, and positive antibodies against Saccharomyces cerevisiae were detected in 70% of patients with CD and 15% with UC. 31,43Recently, a study linked bacterial metabolite interactions with Crohn’s disease activity.41 While it remains unclear if dysbiosis is the cause or consequence of inflammation, healthy siblings of those with Crohn’s disease have been demonstrated to have greater dysbiosis than healthy controls suggesting a causal link of the microbiome in disease risk.20
IBS: pathogenesis involves environmental, psychological, and genetic factors, with a growing focus on gut dysbiosis, particularly its connection to the gut–brain axis. Disruptions in this axis are associated with immune activation and epithelial barrier changes, key contributors to functional IBS symptoms.
IBS patients frequently show reduced gut microbiome diversity, particularly in severe cases and especially in IBS-D. Dysbiosis has been shown to differ amongst the subtypes, however a general trend has been noted with lower levels of beneficial bacteria (Bifidobacterium spp., Lactobacillus spp., Faecalibacterium spp.) and increased pathogens including E. coli, Shigella and Rumunicoccus spp.77,60,51,22Dysbiosis-related microbial compounds may affect neurotransmitters and metabolites levels, contributing to functional symptoms such as visceral pain hypersensitivity and altered gut motility.68One study linked higher E. coli levels to visceral hypersensitivity in mice.56 However, not all studies have been able to showcase these results consistently.
Overlap: Could the gut dysbiosis seen in IBD or IBS lead to the development of each other? This seems a question yet to be answered.
What has been observed is that IBS symptoms are common after acute inflammatory events such as diverticulitis or gastroenteritis. IBD could potentially fall in this category of inflammation, suggesting that IBD is a risk factor for the development of IBS.
It has been observed that the IBD microbiota is characterized by an even lower diversity and increase in inflammatory species in comparison to IBS and healthy population: reduced Firmicutes, reduced Bifidobacteria and increased Bacteroides.63,39Compellingly, in animal models, IBD inflammation does not develop in microbe-free conditions. One study in mice concluded that E.coli could potentially mimic quiescent IBD with IBS-like symptoms such as visceral pain.30
The role of probiotics in the management of symptoms of IBS, IBD and the overlap. What is the evidence?
Lower levels of Bifidobacteria and Lactobacilli are found in IBS and IBD patients compared to healthy controls. Probiotics may ease symptoms by stabilizing gut inflammatory signalling, modulating microbiota, inhibiting pathogens, supporting intestinal barrier function, and producing beneficial compounds. Research of probiotics for IBD or IBS-IBD overlap is limited, but for IBS is vast. Let’s explore the evidence:
IBD: Meta-analyses show mixed results. Some studies suggest probiotics may help induce remission and alleviate symptoms in combination with therapy, particularly in mild-to-moderate UC, while evidence for CD is limited.8,9 The British Dietetic Association (BDA) guidelines suggest certain probiotics, alongside medication, may assist with remission induction in mild UC. Other studies show probiotics did not maintain remission.42,34 A 2017 study linked increased butyrate-producing bacteria to better responses to biologic therapy.1Authorities like British Society of Gastroenterology (BSG) and American Gastroenterological Association (AGA) call for more research.
IBS: Several meta-analyses confirm probiotics are safe and effective for IBS management. Probiotics have demonstrated significant improvements in global symptoms, abdominal pain, bloating, constipation, diarrhoea and more, with symptom relief in at least 50% of individuals and symptoms scores improving from 15% to up to 85% depending on the probiotic strain used and individual inter-variabilities.77,38,76,72,75
The BSG recommends probiotics as a first-line treatment alongside dietary change. Other authorities that also acknowledge their beneficial effects include the NHS, IBS Network, BDA, and World Gastroenterology Organisation. Although no specific probiotic is yet recommended by these organisations, it is suggested that probiotics be trialled for 4 weeks in the first instance to assess any benefit.
Overlap: Research is scarce, but an observational study has shown that probiotics improved bowel-related symptoms and quality of life in patients with UC whose IBS-like symptoms persisted during endoscopic remission.32
What probiotics strains have proven to be beneficial?
Probiotic efficacy is strain- and disease-specific, making it essential to choose the right strain for specific clinical symptoms, as each strain may have unique modes of action and genetic profile.37
IBS
Different meta-analyses have recommended:
- Bacillus coagulans Unique IS-2 (MTCC 5260; Optibac) was among the top results in improving abdominal pain, global symptoms, straining and the Bristol stool scale of IBS-D. Reduction of abdominal pain ranged from 50 up to 85%.38,8,76,72
- Bacillus coagulansMTCC 5856 reduced abdominal pain and bloating72
- plantarum299v reduced abdominal pain severity38
- Saccharomyces boulardiiCNCM I-745 reduced abdominal pain frequency38
- Saccharomyces cerevisiae CNCM I-3856 reduced abdominal pain frequency38
- Lactobacillus acidophilusDDS-1 improved IBS-Symptom Severity Score72
- Three different multi-strain probiotic combinations showed improvements in global symptoms and/or abdominal pain38.
- Different strains of Lactobacillus spp and Bifidobacterium spp that have shown promise in improving IBS include: Lactobacillus acidophilus NCFM, Lactobacillus acidophilus-SDC, Lactobacillus acidophilus DDS-1, Bifidobacterium bifidum MIMBb75, Bifidobacterium Lactis UABla-12, and Bifidobacterium infantis 35624.71
IBD: Recommendations of probiotic strains in IBD is still an area in progress. Evidence includes a variety of RCTs and observational studies. Here we show a few:
- The probiotic Saccharomyces boulardii has shown in a retrospective study to reduce Crohn’s Disease Activity Index69; and in a small pilot trial in UC to help induce remission in 17 patients (68%) alongside medication.18 Larger RCTs are still needed to confirm findings.
- Three RCTs of 8 mixed strains (L. paracaseiDSM 24734, plantarum DSM 24730, L. acidophilus DSM 24735, L. bulgaricus DSM 24734, B. longum DSM 24736, B. infantis DSM 24737, B.breve DSM 24732, S. thermophilus DSM 24731) showed induced remission in UC alongside medication.61,45,64
- RCT of Bifidobacterium longum 536 showed significant reduction in UC disease activity index at 8 weeks supplementation.
While probiotics have shown promise in other areas, there are no studies that show a benefit of probiotics for remission maintenance in CD. For further guidance, the BDA guidelines contain a full list of RCTs and a final statement.
Conclusion: Two Sides of the Same Coin?
While IBS is characterized by recurring abdominal pain and altered bowel habits without visible inflammation, IBD involves chronic mucosal inflammation. Many IBD patients in remission still experience IBS-like symptoms, suggesting a potential co-existence. Research increasingly points to gut dysbiosis as a common risk factor, with both conditions showing reduced diversity and increase in potential pathogens. Probiotics have shown promise in managing IBS symptoms, particularly the strain Bacillus coagulans Unique IS-2. For IBD, probiotics have shown beneficial effects in some cases when combined with standard therapy. Further research is needed to clarify their role in managing the IBS-IBD overlap. Understanding this relationship may help to optimise treatment strategies for these patients.
Written in collaboration with the healthcare professional support team at Optibac Probiotics. Peer-reviewed by Dr Bridgette Wilson.
Disclaimer: This blog has been developed in association with the healthcare professional support team at Optibac Probiotics. Approval of each sponsor and activity is carefully assessed for suitability on a case by case basis. Sponsorship does not imply any endorsement of the brand by MyNutriWeb, its organisers, its moderators or any participating healthcare professional, or their association. Sponsorship funds are reinvested into the creation and promotion of professional development opportunities on MyNutriWeb.
YOU MAY ALSO BE INTERESTED IN:
Probiotics in gut disorders management




