


By Natalie Brabben, Communications Officer, Action on Salt and Sugar
X (formerly Twitter), LinkedIn, Instagram, BlueSky
Salt may be minuscule, but its impact on health is anything but. Despite being proven to raise blood pressure and acting as a major contributing factor to heart attacks and strokes (responsible for 1 in 4 UK deaths!) salt remains the “forgotten killer” of public health. We’ve long known excessive salt is bad for our health, but why are we yet to see permanent efforts to reduce it, and what can we do to finally drive that lasting change?
Introduction
For years salt has been dubbed the “forgotten killer”, hidden in everyday foods, quietly raising our blood pressure and contributing to increased risk of heart attacks, strokes, kidney disease and certain cancers. Despite decades of research and public health campaigns, excessive salt intake remains a persistently overlooked and underestimated problem.
The UK once paved the way in successful salt reduction, yet today, momentum has stalled, reverting the progress once made and putting public health at risk. Many people remain unaware of the fact we’re eating too much salt because the majority (a shocking 75%!) is already in the foods we buy.1 We increasingly rely on manufactured foods, from convenience items to staple goods, and as a result food companies are more responsible than ever for our salt intake. Through surveys that expose the wide variation of salt levels in food categories, Action on Salt have continuously shown salt reduction is possible, so why isn’t our food changing? This Salt Awareness Week we dive into exactly why salt reduction in the UK has stalled and what healthcare professionals can do to reawaken the shakedown of salt.
A Background on Salt Reduction
In the early 2000s the UK emerged as a global leader in salt reduction. Recognising the role of the food industry in determining salt intakes, in 2006 the Food Standards Agency (FSA), who were responsible for nutrition at the time, set about developing a comprehensive salt reduction programme, setting reduction targets for 85 categories of processed foods.2 The FSA oversaw strict monitoring and evaluation of industry progress and reviewed and reset the targets in 2008 to encourage a gradual reduction in salt, that allowed time for consumer tastes to adapt.2
As a result, between 2003 and 2014 salt intake fell from 9.38g to 7.58g a day, decreasing from over 9 sachets of salt to 7.5 per day, and seeing a reduction of 1.8g in just over 10 years.3 As seen on the graph below, this also corresponded with a measured decrease in blood pressure and cardiovascular mortality, scoring a huge win for public health.
However, recent data tells a very different story. In an analysis of blood pressure, cardiovascular mortality, and salt intake measured by 24-hour sodium excretion and national survey data, the most recent figures on population salt intake revealed a concerning rise to 8.39g (8.3 salt sachets or about 1.5 teaspoons), reversing years of success.3,4 This rise signals a disturbing halt in progress, which begs the question, why is the UK failing to reduce salt?
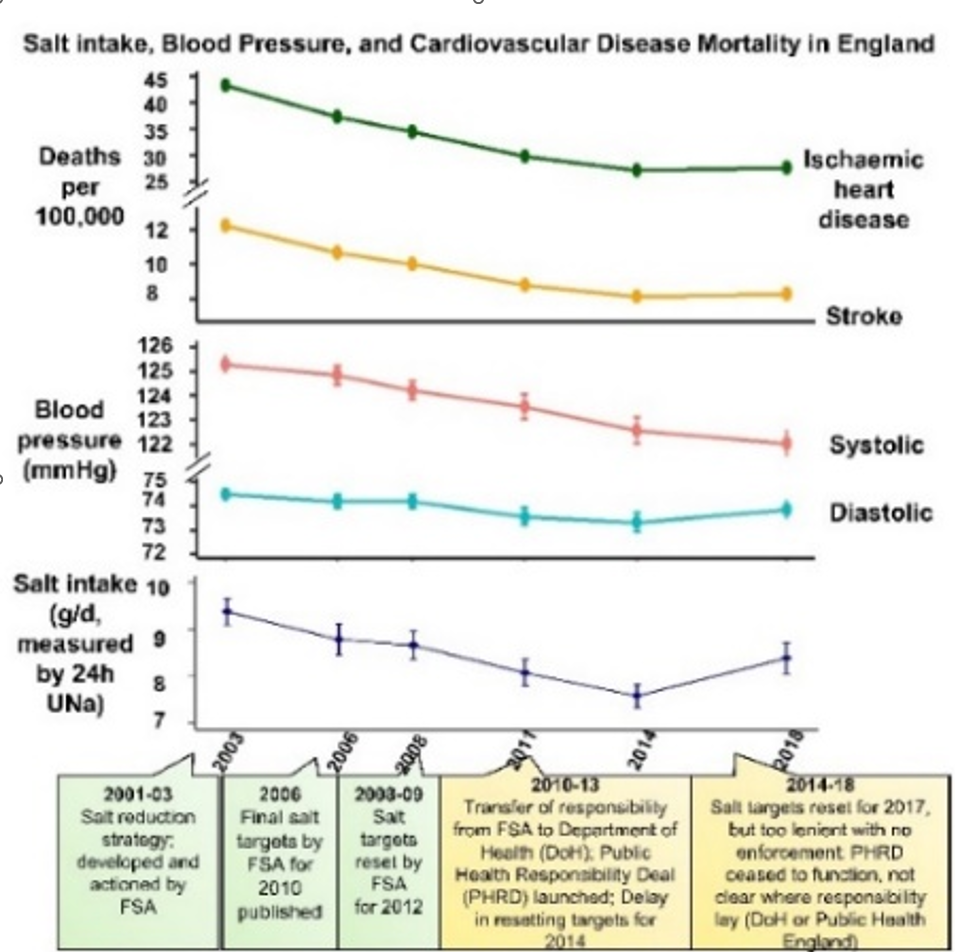
Pictured: Graph demonstrating salt intake, blood pressure, and cardiovascular disease mortality in England from 2001 to 2018.3
Why is the UK failing on salt reduction?
Several factors have contributed to the UK’s salt stagnation.
Shifted responsibility
Under the FSA, salt reduction was a core nutritional priority. Working independently of ministerial control, the voluntary programme under their leadership saw clear and extensive targets, close engagement, and regular industry monitoring.5 However, a decisive shift in reduction efforts came in 2010, when responsibility for nutrition moved away from the FSA to the Department of Health and into its new Public Health Responsibility Deal (PHRD).6 This voluntary scheme placed salt reduction largely in the hands of the food industry itself. With minimal oversight or enforcement and little evaluation of the targets, it became much harder to monitor industry progress and allowed many companies to abandon their reformulation efforts.6
The PHRD was a complete failure and whilst not lasting long, the damage was irreparable.5 When targets were eventually introduced in 2014, the heavy industry lobbying that the PHRD had allowed for led to less stringent recommendations, causing salt reduction to falter further and granting companies less accountability. These issues continued into 2015 with the transfer of responsibility to the newly founded Public Health England (PHE). Under PHE, the salt reduction programme was still recognised but was now absorbed into the ‘sugar reduction and wider reformulation’ programme within the government’s broader Childhood Obesity Plan.7 As a result, industry progress towards the 2017 Salt Targets saw a dismal 52% average compliance from retailers and manufacturers.8
In 2020, PHE renewed the targets with an aim to achieve by December 2024 and committed to a review of industry progress along the way.9 However, they were disbanded shortly after and salt policy moved once again, this time to the Office for Health Improvements and Disparities (OHID), bringing about yet another wave of policy uncertainty and inaction. Five years on and this lack of government accountability continues even today. The promised progress report remains unseen and this current government’s silence on the renewal of the salt targets (whether voluntary or otherwise) suggests a troubling neglect of salt within legislative health policy.
As a result of this decade-long revolving door of responsibility, salt has been pushed to the wayside. The food industry has been able to sideline reform, undoing much of the momentum gained in the early 2000s and accounting for the high levels of salt intake we see today.
A Lack of Mandatory Salt Targets
Over the past two decades, the UK’s salt reduction strategy has relied on voluntary measures, however since its introduction, food manufacturers have failed to fully meet voluntary quotas and have faced no penalty or fallout from doing so.
This failure is twofold; not only is compliance inconsistent across food categories but also varies significantly between companies. While some food categories such as breakfast cereals and breads have seen improvements,10 others such as cheese have seen little reformulation and remain major contributors of salt.11 Business compliance is similarly uneven, with company size, resources, and corporate priorities all determining level of reduction and creating an uneven industry playing field in the process. The issue isn’t technical feasibility, but lack of accountability. With targets and regulations only ever a voluntary measure, there is very little incentive for food businesses, making the policies highly ineffective.
In contrast, the success of the Soft Drinks Industry Levy (SDIL) highlights the capability of mandated measures.12 Introduced in 2018, the SDIL imposed a tax on soft drinks, reducing sugar content by 46% and shifting consumer and industry behaviour. 13 The most recent Autumn Budget14 announcement also saw an uprate to the scheme, keeping it at the forefront of health priority and proving the government can keep fiscal policies aligned with public needs – capabilities that, unfortunately, have yet to extend to salt.
Salt as a Public Health Concern
Although both government and healthcare professionals recognise salt consumption as a public health issue, it often takes a backseat in broader health discussions. Public awareness remains limited and messaging around salt reduction often lacks the visibility and impact of similar health movements, such as anti-smoking campaigns.
Critically, salts direct impact on blood pressure and cardiovascular health is alarmingly underrepresented in media and public messaging, despite circulatory diseases accounting for over one quarter of deaths annually.15 Additionally, despite its effects, excessive salt intake is often regarded as a concern exclusively for older or high-risk populations, limiting the level of priority it’s treated with – and yet with an estimated 5 million people in the UK living with undiagnosed high blood pressure,16 salt reduction has clear benefits for all.
Part of the success of the FSA’s salt reduction programme lay in its multifaceted approach, with strong public awareness campaigns (remember Sid the Slug?) driving an increased understanding from all population groups.17 Much of the problem with contemporary salt reduction remains in the fact the many people are unaware of salt as an issue, a problem that’s heightened through salt’s less observable long-term effects on the body. Salt is a silent killer and when not effectively treated as a public health concern and without stronger public education and awareness campaigns, such as Salt Awareness Week, the risks of high salt intake will continue to be recognised too late.
Pictured: The FSA’s ‘Sid the Slug’ campaign that ran in the early 2000s to encourage public awareness on the impact of excessive salt consumption.17
So, what can we do as healthcare professionals?
Healthcare professionals have a crucial role in driving UK salt reduction forward.
At a policy level, healthcare professionals can advocate for mandatory salt targets and clearer accountability measures. By engaging with policymakers and presenting a clear evidence-base for the health and economic benefits of reduction, such as that in the recent Recipe for Change ‘Incentivising Reformulation’ report and our Salt Awareness Week report, we can help ensure salt stays on the public health agenda.

Within the food industry, healthcare professionals can promote reformulation strategies that reduce salt without compromising taste – for example applying gradual reductions that go relatively unnoticed, using lower sodium salt replacers or decreasing salt crystal size.
At a public level, promoting healthier choices and raising awareness is essential. Whether that’s directly reducing salt, or focusing efforts to prioritise wholegrains, plant-based alternatives, and fresh fruit and vegetables that benefit diets holistically. This year’s Salt Awareness campaign highlights 6 simple actions individuals can take to help reduce their intake to 6g a day:
- Check food labels and choose lower salt options
- Boost flavour and health with herbs and spices in place of salt
- Use low or reduced sodium salts, seasonings and sauces
- Drain and rinse canned vegetables and beans
- Eat mostly fresh, minimally processed foods
- Gradually reduce salt in your recipes
- Through working within the food industry, behaviour change initiatives, and policy support, healthcare professionals can help create a future where salt reduction – and by extension better public health and nutrition – is a public health priority and a practical part of everyday life.
Conclusion
The evidence is clear, salt reduction is one of the most effective ways to reduce the risk of cardiovascular disease, stroke, and other major health conditions. Without stronger government intervention, clear mandated regulations, and greater accountability across the food sector, salt reduction progress will remain stalled. With public health now more of a concern than ever, it’s time for salt to start being treated with the urgency it demands.
References
- NHS. Salt in Your Diet. NHS. Published April 17, 2023. Accessed April 15, 2025. https://www.nhs.uk/live-well/eat-well/food-types/salt-in-your-diet/
- Food Standards Agency. UK Salt Reduction Initiatives. https://webarchive.nationalarchives.gov.uk/ukgwa/20131206171601/http://www.food.gov.uk/multimedia/pdfs/saltreductioninitiatives.pdf. Published 2013. Accessed April 23, 2025.
- Song J, Tan M, Wang C, Brown M, Pombo-Rodrigues S, MacGregor G, Feng H. Salt intake, blood pressure and cardiovascular disease mortality in England, 2003–2018. Journal of Hypertension. 2023; 41(11). https://pubmed.ncbi.nlm.nih.gov/37723900/
- Public Health England. National Diet and Nutrition Survey. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/876252/Report_England_Sodium_Survey_2018-to-2019__3_.pdf. Published March 2020. Accessed April 15, 2025.
- MacGregor G, Feng H, Pombo-Rodrigues S. Food and the Responsibility Deal: How the Salt reduction Strategy was Derailed. The BMJ. 2015;350. doi: https://doi.org/10.1136/bmj.h1936
- Department of Health and Social Care. Public Health Responsibility Deal. Gov.UK. Published July 25, 2011. Accessed April 15, 2025. https://www.gov.uk/government/news/public-health-responsibility-deal
- Department of Health and Social Care. Childhood Obesity: A Plan for Action. Gov.UK. Published January 20, 2017. Accessed April 15, 2025. https://www.gov.uk/government/publications/childhood-obesity-a-plan-for-action/childhood-obesity-a-plan-for-action
- Public Health England. Salt Targets 2017: Progress Report Summary. https://www.gov.uk/government/publications/salt-targets-2017-progress-report/salt-targets-2017-progress-report-summary. Published January 2019. Accessed April 15, 2025.
- Public Health England. Salt Reduction Targets for 2024. https://assets.publishing.service.gov.uk/media/5f5618c8d3bf7f4d75de6ff1/2024_salt_reduction_targets_070920-FINAL-1.pdf. Published September 2020. Accessed April 15, 2025.
- Public Health England. Salt Targets 2017: Second Progress Report. https://assets.publishing.service.gov.uk/media/5f5610a98fa8f535ecce099c/Salt_targets_2017_Second_progress_report_031020.pdf. Published September 2020. Accessed April 14, 2025.
- Action on Salt. Cheese Industry Showing no Signs of Salt Reduction New Study Shows. Action on Salt. Published March 8, 2024. Accessed April 14, 2025. https://www.actiononsalt.org.uk/salt-surveys/2024/cheese/
- Sasse T, Metcalfe S. Sugar Tax. Institute for Government. Published November 14, 2022. Accessed April 14, 2025. https://www.instituteforgovernment.org.uk/explainer/sugar-tax
- HM Treasury. HMT-HMRC Soft Drinks Industry Levy Review. https://www.gov.uk/government/publications/soft-drinks-industry-levy-review/hmt-hmrc-soft-drinks-industry-levy-review. Published October 30, 2024. Accessed April 15, 2025.
- HM Treasury. Autumn Budget 2025: Fixing the Foundations to Deliver Change. https://assets.publishing.service.gov.uk/media/672b9695fbd69e1861921c63/Autumn_Budget_2024_Accessible.pdf. Published October 30, 2024. Accessed April 15, 2025.
- British Heart Foundation. UK CVD Factsheet. https://www.bhf.org.uk/-/media/files/for-professionals/research/heart-statistics/bhf-cvd-statistics-uk-factsheet.pdf. Published January 2025. Accessed April 14, 2025.
- British Heart Foundation. High Blood Pressure. British Heart Foundation. Published March 2023. Accessed April 14, 2025. https://www.bhf.org.uk/informationsupport/risk-factors/high-blood-pressure
- Action on Salt. Salt Reduction: What Works?. https://www.actiononsalt.org.uk/media/action-on-salt/awareness/shake-the-salt-habit2022/AoS-and-WASSH_Salt-Reduction-What-Works.pdf. Published March 2022. Accessed April 15, 2025.




